I like this. A lot. I’ll be sending it to several people. Thanks!
In an attempt to redeem myself, here’s a link to a BBC podcast called More or Less (an excellent maths based programme)
It has 3 items of which I found 2 very interesting
- Statistical analysis of the covid19 rate of deaths compared to the annual death rate in the UK
- An attempt to math out the likely number of cases in Iran as compared to the reported numbers
So regarding death rates:
It’s been posited, via the Italian town analysis and anecdata from France and other countries that the true mortality from coronavirus is much higher than recorded in official stats in most countries. I though we would have to wait to see a statistical mortality analysis, but apparently not.
Turns out Spain has an active mortality monitor. This is the latest data:
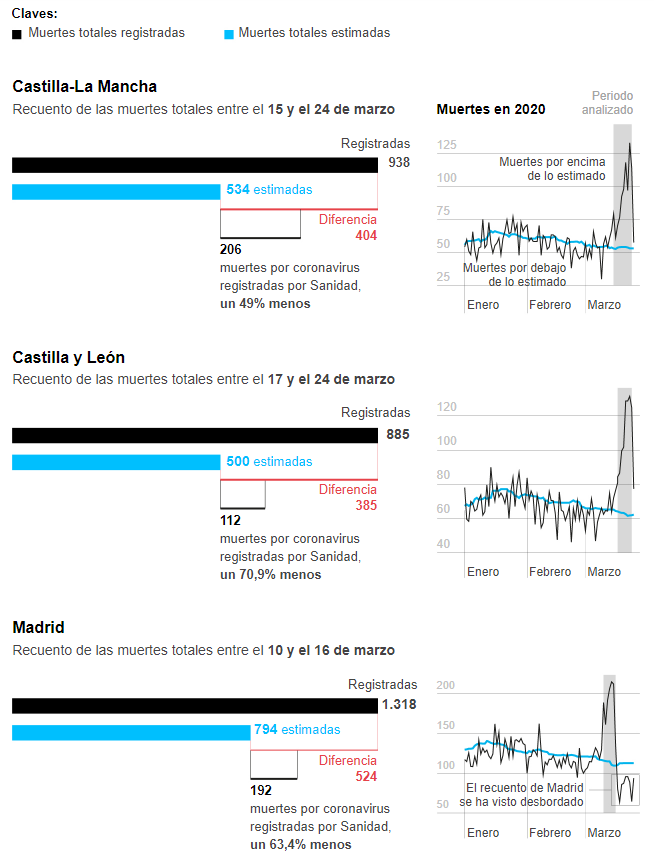
So yeah, we can see a quite high excess mortality. That was to be expected (Madrid dip at the end is because of collapse in the reporting).
We can also see excess mortality is about twice the recorded deaths due to COVID-19.
This is basically deaths of untested individuals, most of them unidentified as cases before death. Since the individual is not tested and you don’t test corpses because you can’t spare tests, those go unrecorded.
Source: https://elpais.com/sociedad/2020-03-27/el-coronavirus-causa-mas-muertes-de-las-detectadas.html
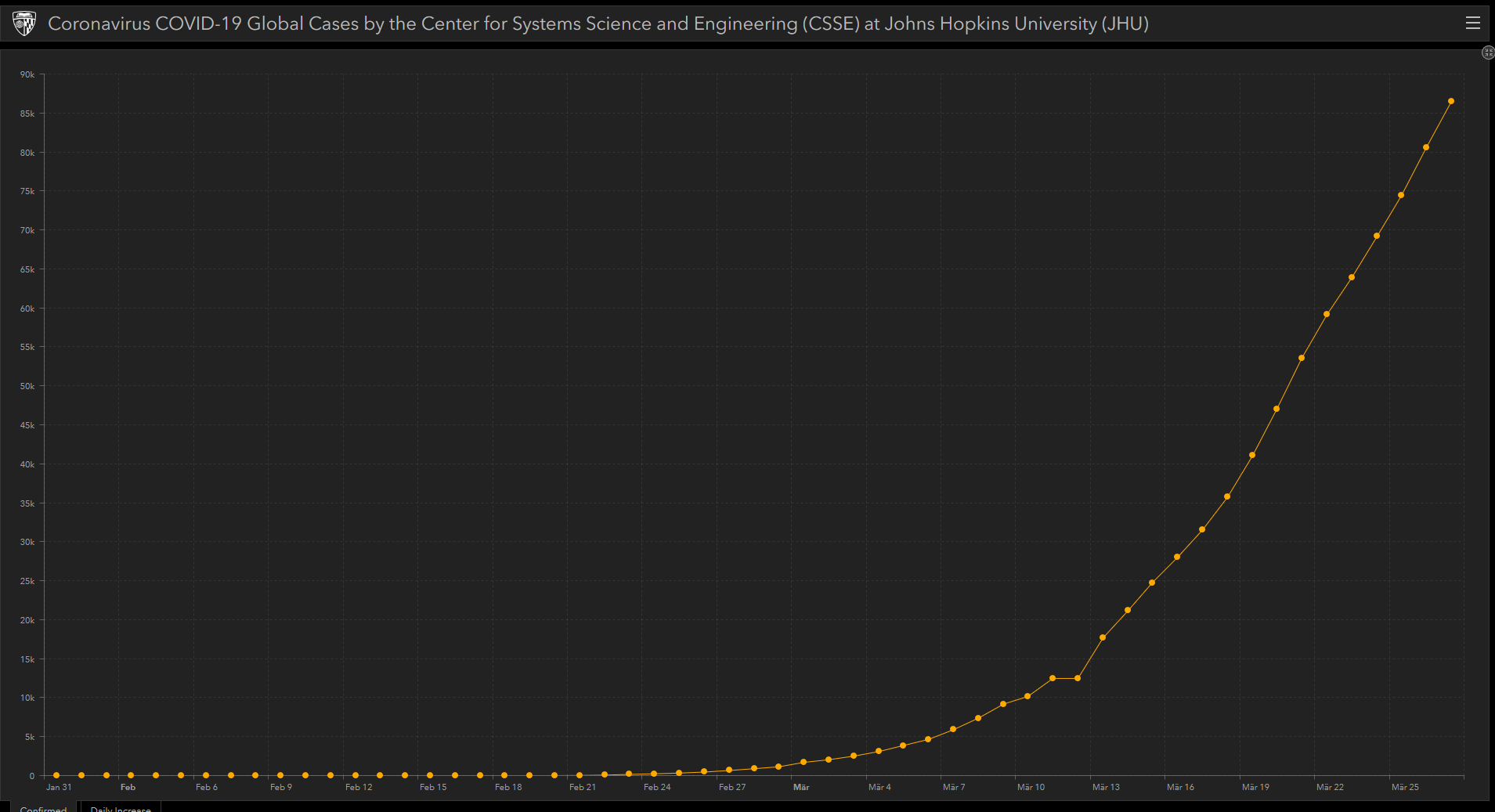
This is the Italian graph of total infections. Am I right to think that it is not exponential growth anymore but more of a steep linear growth? Is this the best we western countries can do? (I hope I am posting in the correct thread)
Italy has been on a linear growth for cases and deaths (although yesterday there was an spike in deaths) for some days now.
They did make the measures even more strict a week ago or so (I think, unclear about the timing at this point) so hopefully those new measures can nudge the curve into a decrease of new cases/deaths soon.
Convince me it’s not a lack of testing. I still think most countries are only testing a limited number of people - for example here in the states, there were so many preconditions on getting tested, that when they finally do test, those people are sick and you’re going to get more people dying from that tested population.
So for example, if we look at Italy with 92,472 cases + 10,023 deaths, if we use mortality of 2.0, we have cases three weeks ago = 10,203 / 0.02 = 501,150 and with a doubling every 3.5 days, the number of actual cases today is 5,669,865.
So is the mortality higher or more cases being missed? This is the question that keeps coming up.
Regarding testing, what does this mean? Is it really that hit or miss or is something else going on? Because that is not comforting at all.
Sorry, I meant raw deaths, not mortality. We won’t know real mortality until statistical analysis with random samples of the population are made to ascertain the real reach of the epidemic.
But my data referred to people dying that were not tested, and thus the raw death numbers being higher than the official count, in this case by about 2x.
People are assuming death counts are one of the most accurate numbers to see reach of infection, given than test numbers vary according to regime. This data shows that even death numbers can be wildly off depending on how you count. For example, France has not counted any person who died at an assisted living facility and only counted deaths at hospitals. They are going to start correcting for that, but overall it seems in a lot of places many deaths are being missed.
Spain has far higher mortality on a per case basis. And when contemplating these numbers, here are the factors I believe could play into that:
-demographic spread of infected population (Spain median age is higher, more smokers perhaps?). We definitely saw a mortality spike in Seattle due to infected populations initially favoring nursing home residents.
-healthcare capacity. Though the US has passed Spain in cases, the US is vastly larger and so has greater capacity. As the infection grows here I would sadly not be shocked to see an increase in mortality here as capacity is reached in localized pockets. NUC would be the first evidence of this
-timing. There appears to be some lag between infection and death. Spain cases started growing before they did in the US. Ergo they may be further along the curve, and we might see growth in mortality as the situation evolves here.
-testing. Maybe we are testing more cases? Or maybe testing less dead patients who were not confirmed prior. Either one could lead to fewer deaths per case.
I am not ascribing it to any one factor, or excluding factors not listed. But the US has about a 1.5% fatality on cases at current (this will grow, simply due to lag in positive and death). Spain is sitting at 8%. That is a huge difference and indicates there is something very different with the way the numbers are tabulated.
Edit: yeah, also the mentioned above examples of simply not counting certain cases, such as not counting nursing home deaths in France.
Ah, great. Thanks. Makes sense.
Again, that’s rates. What I mean is that most likely Spanish deaths are quite higher than reported and mortality rate probably at 15% or so.
The higher mortality rate is mostly due to an aging population (a lot of spread in elderly assisted living facilities) and testing deficiency (although that’s improving and we are now testing 20k daily, it’s going to take a while to catch up). We know there were about 55k suspected but not tested cases in Madrid on March 25th.
As far as I know, the healthcare system is at a stress, but has not reached full saturation and there were ICU beds and ventilators available in Madrid at least two days ago (when I just heard). So this is probably having some impact in mortality, but it’s probably minor compared to the two other cases, at least for now.
Yeah makes sense. Its hard enough tracking US updates, let alone Spanish. So testing deficiency makes sense.
Also yeah, I fear we are going to start discovering the statistical distinction between healthcare systems under and over capacity and fatality rates. Hooray for natural experiments ☹️
This number I think was based on Chinese data. Now that we have seen Covid in numerous other countries, The chinese data becomes really hard to believe as accurate as far as death rate anyway. Germany though, remains an outlier among European countries.
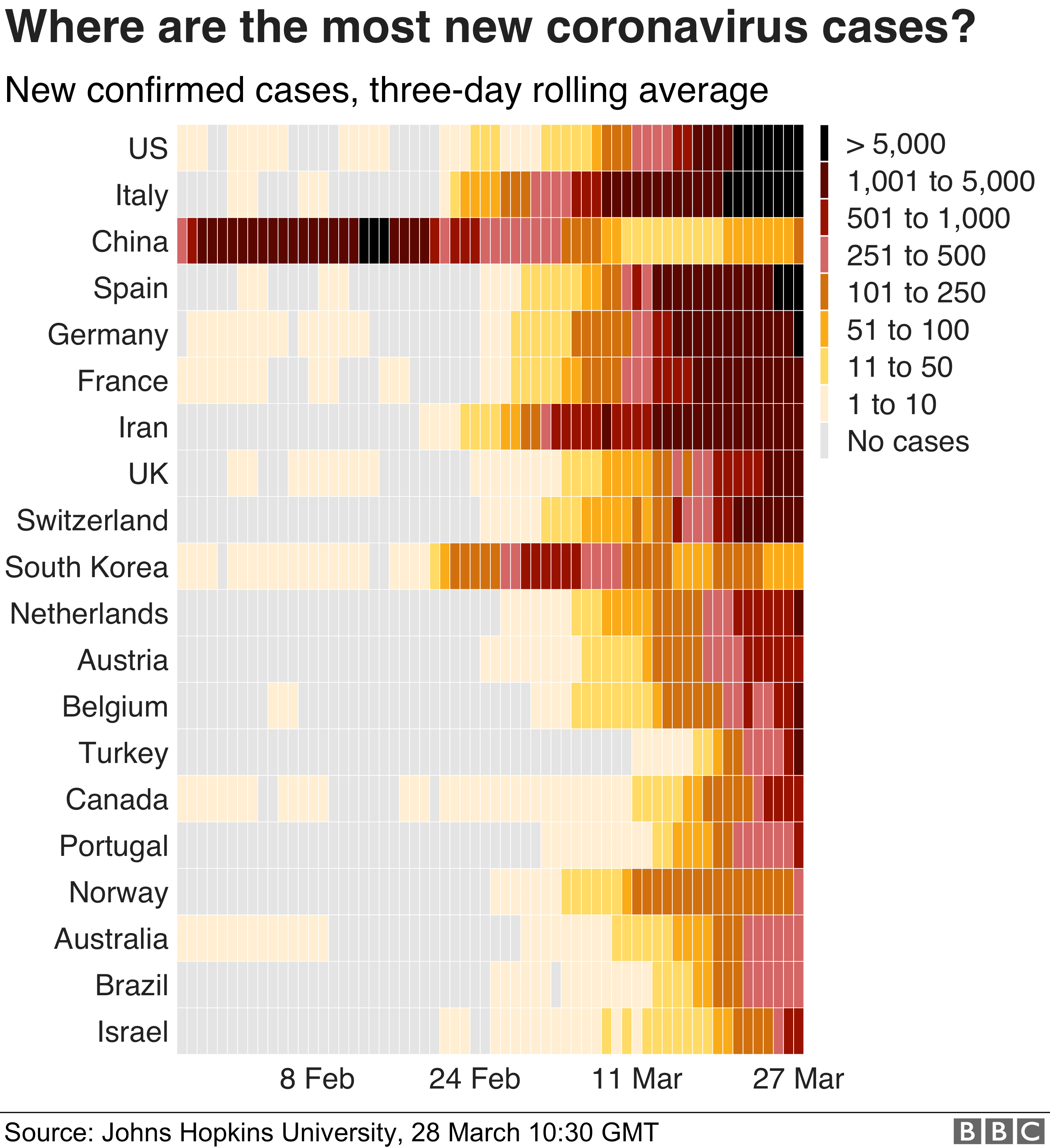
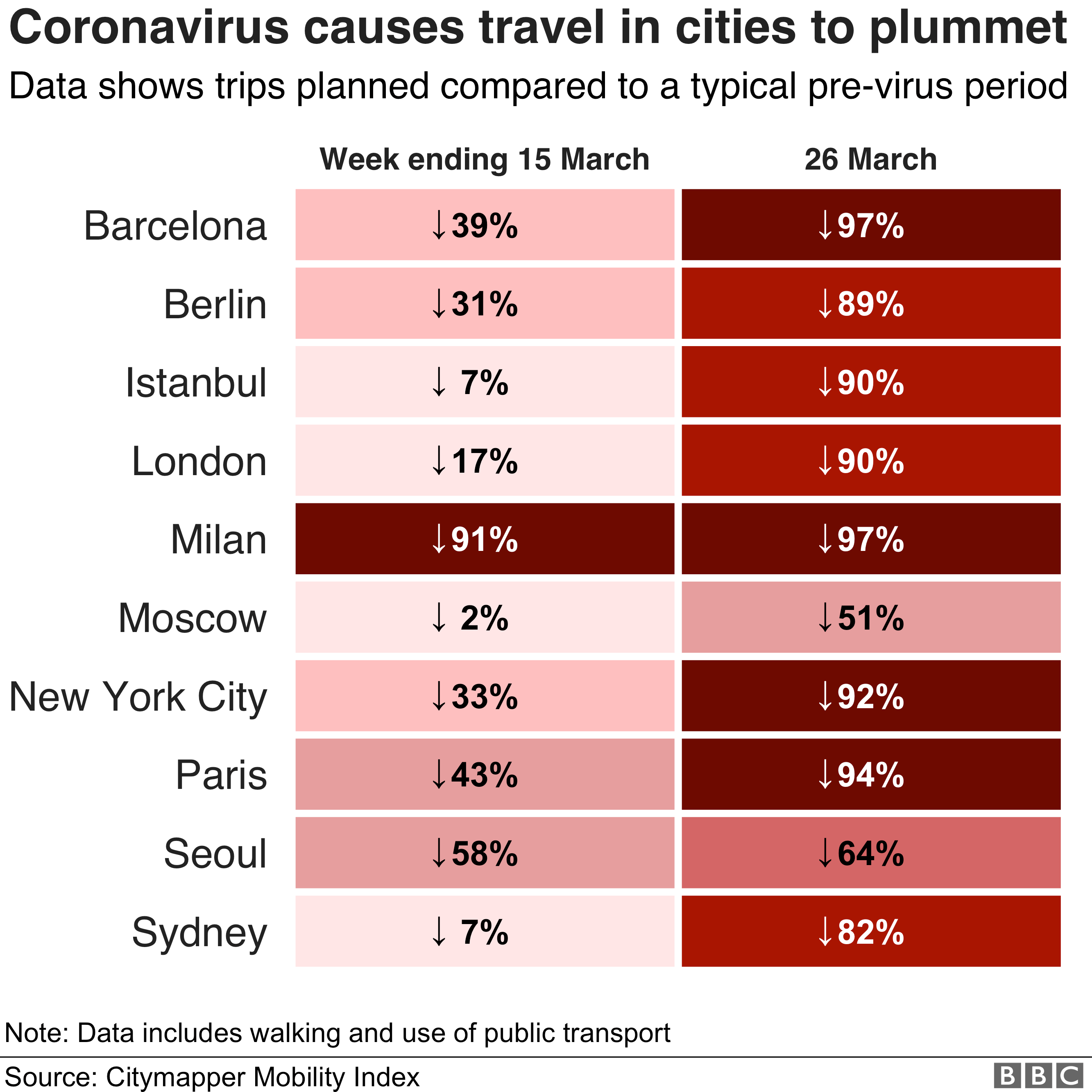
The BBC has a series of interesting graphs to visualise the evolution of the Pandemic here:
Among those:
This one showing the later lock downs for some locations:
And this one explaining maybe why, for many Americans, it’s not a problem, just another flu outbreak:

It doesn’t matter what you have the mortality as, it’s just illustrative. Eg, plug a mortality rate of 1.0 and the # of cases doubles, make it 4 and it halves - the point being that the number of actual cases still exceeds the reported cases by a huge amount.
Another really good episode with an expert who is infected and is advising dr. Fauci
I agree. I apologize, as I simply wanted to use the opportunity to question the chinese numbers now that we have more data from more (reliable?) countries, and didn’t make that very clear.
Given their testing regime, the South Korean mortality rate is probably the nearest to anything we have approaching a reasonable guesstimate of the mortality rate
It means that until we can get some actual data and tests to examine, it’s a news story and not actual data. It’s anecdote.
There have been isolated incidents of similar reports from time to time, but the amount of data we’re seeing on recovered patients suggests that this is either super rare, or caused by some procedural error at this point.
If it helps set your mind at ease, virologists who’ve spent a lot of time in the last two months looking at this virus and studying how it behaves are pretty confident that humans develop immunity to the virus after recovering from infection.
From a Wikipedia article: https://en.wikipedia.org/wiki/Health_in_South_Korea:
Life expectancy has been rising rapidly and South Korea ranked 11th in the world for life expectancy in 2016.[1] South Korea has among the lowest HIV/AIDS adult prevalence rate in the world, with just 0.1% of the population being infected, significantly lower than the U.S. at 0.6%, France’s 0.4%, and the UK’s 0.3% prevalence rate. South Korea ranked highest in influenza vaccination in Asia at 311 vaccines per 1,000 people.[2]
A new measure of expected human capital calculated for 195 countries from 1990 to 2016 and defined for each birth cohort as the expected years lived from age 20 to 64 years and adjusted for educational attainment, learning or education quality, and functional health status was published by the Lancet in September 2018. South Korea had the sixth highest level of expected human capital with 26 health, education, and learning-adjusted expected years lived between age 20 and 64 years. [3]
Obesity has been consistently among the world’s lowest - only 3% of the population were obese, which was the second lowest in the OECD, compared to over 30% in the U.S. or 23% in the UK.[4] As a result, mortality from cardiovascular disease was the fourth lowest in the OECD.[5][6]
So they really seem to represent a best case scenario. Good health in general, excellent healthcare system, and excellent testing and response to Covid-19.