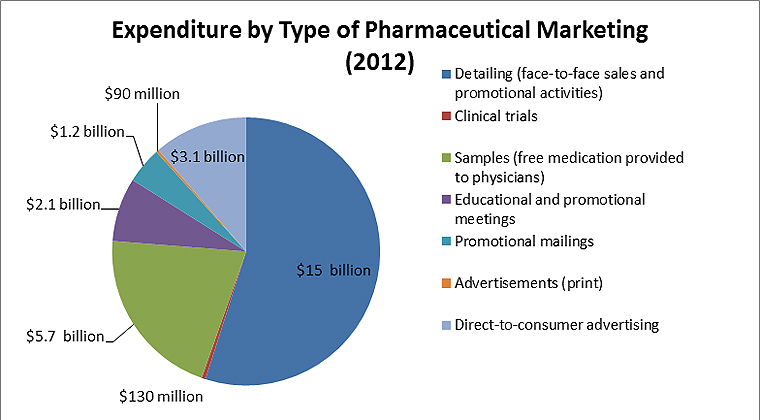
Nesrie, Pharma spent $24 billion marketing to healthcare professionals in 2012. $3 billion went on marketing to the general public.
The way the Pharma industry markets to physicians is both immoral and unethical. That it isn’t illegal is a damning fucking indictment of the US Healthcare system and legislation concerning it.
Among other things they subvert (largely) well meaning and well intentioned healthcare professionals into becoming brand ambassadors, even when the evidence available to professionals is that the drug in question has limited efficacy (or is less efficacious than a generic or cheaper alternative). I can’t find any articles on it, but there are plenty that go into great detail on just how insidious and wrong Pharma marketing is in the US.
This quote is from a decade ago;
[quote]Most of this is spent on advertising to doctors. Drug companies spend a great deal of time deciding how many calls to make to each individual physician and when to make those calls. Narayanan’s third research project thus went into greater depth in studying the effectiveness of these efforts.
Not surprisingly, the study found that doctors learn at different rates: There are fast learners, slow learners, and those who fall in between. But currently, drug makers tend to divvy up their detailing dollars based upon whether physicians are heavy prescribers or light prescribers—not on how quickly they understand the nuances of a particular drug. “And, if you persist in detailing information about a particular drug to a fast learner, your marketing dollars are effectively wasted,” said Narayanan. On the other hand, stopping your detailing before a slower learner has absorbed everything he or she needs to know about a particular drug can end up hurting overall sales.
Pharmaceutical firms can distinguish fast learners from slow learners through statistical analyses such as how quickly a doctor prescribes a new drug based on his or her age, time since graduation from medical school, or other attributes that can be easily observed. There are consulting firms in the industry that perform these types of analyses to help drug makers target their detailing more precisely, said Narayanan.[/quote]
Does that not frighten you? What kind of statistical methods are they using now to profile HCPs to figure out which can be ‘educated’ into using their pharmaceuticals? And how much money needs to be involved in the education?